What triggers normal, full-term labor is not yet fully understood, so the actual cause of preterm labor is not completely understood. In over half of preterm labors, the cause is unknown. However, there are some factors which are known to increase a woman’s risk of experiencing preterm labor.
Many preterm births (30-40%) are the result of preterm premature rupture of the membranes (PPROM), in which the amniotic sac that holds the baby breaks too soon, leading to preterm labor. Preterm labor usually begins shortly after PPROM occurs. Sometimes, when a slow leak is present and infection has not developed, contractions may not start for a few days. On occasion, a leak high up in the amniotic sac may reseal itself so that preterm labor does not start or subsides.
A mother’s age may play a role in preterm labor. Women in their teens or women over 35 are at an increased risk. Also, some recent studies have found a link between severe stress and stressful life situations (including things like: domestic violence or death of a close family member) and preterm labor, as well as standing for long periods of time or extremely tiring jobs.
Infections can cause preterm labor, including certain sexually transmitted diseases (STDs) such as: gonorrhea, syphilis, chronic active hepatitis, trichomoniasis and chlamydia, as well as any illness with a fever. Severe urinary tract infections (UTI), undetected or untreated, Group B Strep and bacterial vaginosis (BV) are also possible triggers of labor before term. Other conditions that may be related to preterm labor include certain chronic maternal illnesses such as: diabetes, high blood pressure, kidney disease/infection and sickle cell anemia.
Illegal or non-prescription drug abuse (especially cocaine), cigarette smoking, alcohol consumption are all risk factors for delivering a preterm baby. Not gaining enough weight during pregnancy, having a pre-pregnancy weight of less than 100 pounds, and inadequate nutrition and prenatal care may cause preterm labor and delivery of a premature infant.
A multiple pregnancy (expecting twins, triplets or more) puts you at a much higher risk for preterm labor. The increased size of the mother plays a role in the increased risk. Women who’ve had a previous preterm labor or premature baby, 3 or more first-trimester miscarriages or 1 second-trimester miscarriage are considered at a higher risk as well.
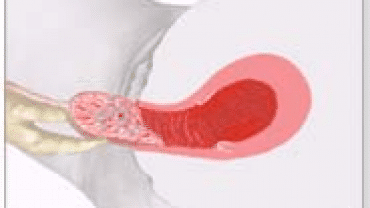
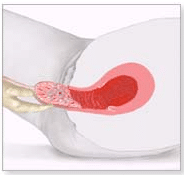
Cervical trauma is a major cause for preterm birth, the most common being from cervical injury due to elective abortions. Women with a history of multiple first-trimester abortions or one or more second-trimester abortions are at a considerably increased risk of delivering before term. Uterine defects due to an incompetent cervix, uterine fibroids, excesses amniotic fluid (making the uterus extra large), previous cervical cone biopsy surgery, placenta previa and diethylstilbestrol (DES) exposure can lead to preterm labor, as well as a pregnancy that occurred while using an IUD (contraceptive device).
Back to Labor Stages

 Prematurity is the most common cause of sickness and death among newborns. Babies born before the 37th week of pregnancy are often called preterm or “premature”, babies born before the 32nd week are considered very premature, babies born before the 28th week are considered extremely premature. Generally, babies born after the 25th week of pregnancy have a survival rate of between 50-60% (although they will stay an extended period of time in intensive care), which increases dramatically to over 90% after the 28th week.
Prematurity is the most common cause of sickness and death among newborns. Babies born before the 37th week of pregnancy are often called preterm or “premature”, babies born before the 32nd week are considered very premature, babies born before the 28th week are considered extremely premature. Generally, babies born after the 25th week of pregnancy have a survival rate of between 50-60% (although they will stay an extended period of time in intensive care), which increases dramatically to over 90% after the 28th week.